
Using situational awareness to identify the first principles of high quality clinical decisions.

The most common approach to tackling the question of how to foster shared decision making in routine clinical care is to identify barriers impeding its adoption. Commonly identified barriers include: health systems do not view shared decision making as the standard of care, insufficient time during patient visits, poor fit into the clinical workflow, paucity of appropriate information, and that clinicians find shared decision making difficult to accomplish. [1] Although these barriers have been known for some time, little progress has been made in overcoming them. [2]
In recent Musings, I suggested taking a First Principles Thinking approach to creating a new, more effective clinical decision making method that recognizes the importance of patient involvement in decisions about their health, i.e., shared decision making. First Principles Thinking is designed to encourage new approaches to resolving stubborn problems. The underlying premise is that starting from scratch by concentrating on what needs to be accomplished, what the basic elements involved are and how they can be effectively organized is more likely to succeed that continually trying to tweak the status quo.
With regard to fostering the adoption of shared decision making in clinical practice, I think the goal is to improve the overall quality of the clinical decision making process. This goal includes routine use of shared decision making when appropriate and also seeks to improve the quality of all aspects of the clinical decision making process. The First Principle irreducible elements can be divided into two big categories: those related to the decision making process and those related to the clinical environment.
From this perspective, the concepts of Situational Awareness, as described by Endsley, provide a useful guide to the both of these categories. [3] I presented an adapted Situational Awareness model for clinical shared decision making in the November 4, 2022 Musing. For this discussion, I’ve left the shared decision making/situational awareness components the same but added a new set of system factors and several new links showing how the clinical practice environment affects elements of the decision making process:
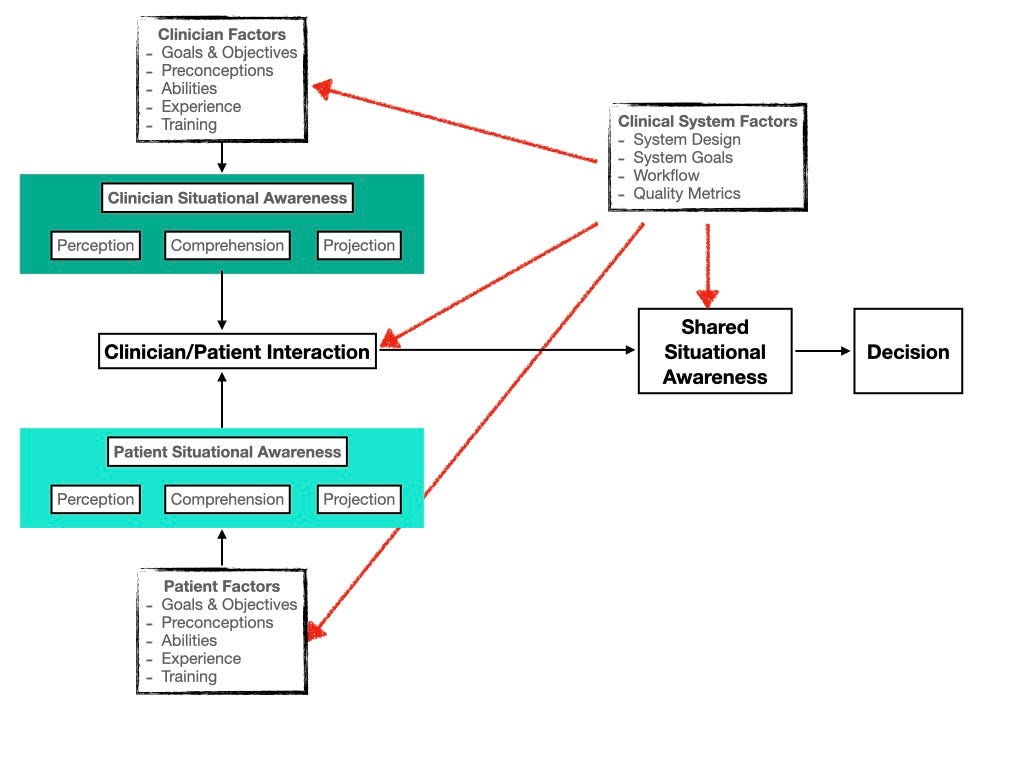
This model identifies several First Principle elements and the interactions among them within a clinical decision making system. Both provider and patient need to achieve an appropriate level of situational awareness about the decision under consideration. This process involves recognizing that a decision needs to be made, achieving a good understanding of the decision parameters (the goal, the options, and the factors important in choosing a preferred option), and considering the likely outcomes of each option. For both parties, how well they can achieve an appropriate level of situational awareness depends on what they are trying to accomplish and their experience, how well they can access needed information and effectively process it, and decision-making skill. They also need to be able to work together to effectively create a shared situational awareness that will result in making a high quality decision. (I described decision quality using the decision quality chain in the November 18, 2022 Musing.)
The ability of the clinical decision makers to achieve individual and shared situational awareness is also a function of the environment they are working in, i.e., the local clinical microsystem as well as the more widespread healthcare macrosystem. Systems with an underlying goal of improving the quality of clinical care would ensure that patients and providers have the information, time, and training necessary to achieve adequate levels of individual and shared situational awareness and use it to make a high quality decision.
Musings
My proposed model is definitely a work in progress. Nevertheless, I think it presents a good overview of how a better clinical decision making system could be created. I pose it to stimulate further thought and discussion. Note that a system like the one proposed would alleviate the most commonly cited barriers to shared decision making, but depends on a general system-wide approach very different from one based primarily on tweaking the way clinicians discuss care decisions with their patients.
Is a system like this feasible? I believe it is. There is a large trove of resources available that could be used to implement it that have not been introduced into clinical care. It’s time we started doing so. I discussed some of these approaches in the December 2, 2022 Musing.
I will present more details about the use of the decision quality chain as a metric for assessing decision quality in a future Musing.
References
1. Elwyn G, Durand MA, Song J, Aarts J, Barr PJ, Berger Z, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891.
2. Finset A, Street RL. Shared decision making in medicine – improving but still a work in progress. Patient Education and Counseling. 2022 May 1;105(5):1055–6.
3. Endsley MR, Jones DG. Designing for Situation Awareness: An Approach to User-Centered Design, Second Edition. 2nd ed. 2012;396.